|
It is most interesting to
observe the progress made during the first year of the operation of
National Insurance and to survey the actual progress with the criticism
of its opponents well in mind.
In the first place the
National Insurance Act was entirely experimental in this country. No
precedents could be invoked. The Act was necessarily complex in its
manifold details, although exceptionally wide powers were delegated to
the Insurance Commissioners in the shape of administrative, supervisory
and judicial functions. The Insurance Act directly touched the action of
nearly one-third of the entire British population, or some fourteen
millions of people. Not only was it enacted that weekly sums had to be
paid by or on behalf of these people, but their employers had also to
pay contributions and to perform weekly duties in respect of the
collection of the same. Both employers and employees had specific and
frequent duties laid upon them for active and individual observance. The
central administration had to organise an entirely new department of
work and procure and educate its staff. Advisory Committees had to be
formed. Insurance Committees had to be set up for each district.
Approved Societies had to be recognised and set in motion. A medical
service had to be instituted for each part of the country. The provision
of drugs and medicines had to be made. The public in general had to be
informed and educated as to the provisions of a new and complicated Act
of Parliament which cut in every direction into the life and duty of the
nation. In addition to all the difficulties inherent in the sheer
magnitude of this herculean task, destructive and querulous criticism as
to the merits of the Act, and more particularly as to some of its
details, had to be met. ,
An Act which should never
have been allowed to drift into the arena of party politics became a
bone of contention in the press and country, and every bye election
during the past year was fought not on the merits of the Act as a great
social engine of reform, but by party politicians exploiting any and
every grievance that any section of the community felt with regard to
any part of it. In addition to all the difficulties and opposition
engendered by different causes, the medical profession for a variety of
reasons avowed much dislike for and displayed violent opposition to the
conditions appertaining to medical service under the Insurance Act.
Resistance Leagues were formed to work against the Act and a malignant
and persistent opposition press fulminated daily against National
Insurance. The difficulties connected with starting the Act were so many
and the obstacles were so great that many people believed that the Act
would never start, or that if it did begin it would only be partially
operative and that a feeble beginning would end in an ignominious and
early break down. Prominent politicians publicly prophesied that the Act
would never begin. Others said it would not start inside three years.
Others pledged their reputations that it would be five years before half
the insured population would be in Approved Societies. Many others said
and believed that the deposit contributor class would consist of 10, 15,
20, 25 and up to 33% of the insured population.
No Act of Parliament was
ever launched amidst so many difficulties and against such hostile and
menacing opposition.
No Act of Parliament ever
achieved such magnificent and instantaneous administrative success.
The Commissioners threw
themselves with energy and ability into their gigantic task. Staffs were
organised. Leaflets and circulars by the million were printed and
circulated. Lectures were delivered to Societies and the public all over
the country. Advisory Committees were formed. Insurance Committees were
set up and quickly got to work. Societies of every kind were approved
and started operations in the most energetic and fruitful fashion.
Employers everywhere signified that they would obey the law, and many of
them, while keenly critical of the provisions of the Act, evinced great
interest in the work of the Approved Societies and the Public Health and
Tuberculosis crusade under the Act. The mass of the people joined some
kind of Approved Society, and only a very small proportion, for one
reason or another, drifted into the Post Office. The doctors, induced
probably by extra Government grants, took service under the Act. The
rods of the Resistance Leagues withered up and those of the Act
blossomed like Aaron’s. The National Insurance Act in its main great
outlines had come to stay and its successful initiation is at once a
triumphant testimony to the belief of the people in a national system of
insurance against ill-health, and a tribute to the fruitful labours of
those who are working for the prevention and cure of sickness, for the
healing of the nation, and for deliverance from the scourge of the white
plague. The common-sense and law-abiding instincts of the British people
provided a colossal rebuke to the meaner spirits who guided an
unscrupulous agitation against a great scheme for the national welfare.
To Mr. Lloyd George, as
he watched the fate of his child, the months must have been anxious
ones. But he won through in a great triumph. It was after the storm in
his native woods that he sought for and gathered ample stores of
firewood. And now, after the tempest of criticism, he is gathering- the
gratitude of hundreds of his fellow citizens, secured as they never were
before against all that menaces their health and consequently their
comfort. He is almost in the enviable position of the man who makes the
songs of a nation.
In connection with the
initiation of the Act, it should be remembered that Sanatorium benefit
was the only benefit which was immediately operative in July, 1912.
During' the first year, in the United Kingdom, nearly 20,000 persons
received the benefit of some kind of treatment in connection with
Tuberculosis. More definite information for a portion of the year is
contained in a table which is taken from official sources and which is
incorporated in these pages.
Medical benefit began to
operate in January, 1913, and since then on the average in the United
Kingdom nearly 500.000 persons have received medical treatment and
attention every week.
Sickness benefit started
in January, 1913, and on the average in round figures 270,000 persons
have received weekly sick pay in the United Kingdom.
Maternity benefit also
began in January, 1913, and nearly 18.000 maternity benefits have been
paid weekly.
In six months a sum
approaching 2,500,000 has been paid in treating insured persons who were
receiving medical benefit. In the same period nearly two-and-a-half
millions have been disbursed in payment of sickness claims. In half a
year nearly half a million of maternity benefit has been paid.
PROGRESS OF THE ACT IN
SCOTLAND.
The following details are
taken from official sources of the actual progress made in initiating
the National Insurance Act in Scotland :—



Sale of Stamps.
The amount received from
the sale of health insurance stamps in Scotland up to the 11th July was
;£2,040,000. To these receipts there would fall to be added Government
grants both special and those of two-ninths (or one-fourth) of the cost
of benefits and administration.
Expenditure upon
Benefits, etc.
The Amount advanced by
the Scottish Insurance Commissioners to Approved Societies up to 15th
July was ,£710,604, of which ^'4-16,810 was for benefit and ^263,794 for
administration. Advances to Insurance Committees totalled ^'322,992. The
amount paid in respect of claims by deposit contributors up to the same
date was £377 in sickness and ^85 in maternity benefit. It will be
observed from the foregoing figures that the average claim for sickness
and maternity benefit by deposit contributors has been only 3d. per
head, a shrewd comment on those critics who promised us a welter of poor
lives in this section of the scheme.
IV. INSURANCE COMMITTEES
IN SCOTLAND.
The number of Committees
and their aggregate membership may be summarised as follows :—

The number of burgh
Committees is now twenty-five, owing to the Committees for the burghs of
Govan and Partick having ceased to exist in consequence of the recent
extension of the boundaries of the city of Glasgow.
One result of the
constitution of Insurance Committees is a considerable accession to the
number of persons interested in the local administration of the country.
To the extent of one-fifth the members were already members 'of Town and
County Councils. But, as regards the rest (2,000), it may be assumed
that a large proportion had not previously served on any public local
bodies.
V. MEDICAL BENEFIT IN
SCOTLAND. Formation of Panels.
On the 15th January,
1913, when medical benefit came into operation, there were local
difficulties still remaining for adjustment, to which reference will be
made; but in Scotland generally the panels constituted were 'adequate,
and were capable of affording competent medical attendance and treatment
to insured persons.
Further additions were
made to the members on the medical lists during the early weeks and
months of 1913. The following table shows the number of practitioners on
Scottish Panels as at March, 1913, together with the average number of
insured persons per practitioner for each Insurance Committee.
Practitioners on
Medical Lists, Scotland, at March, 1913:—
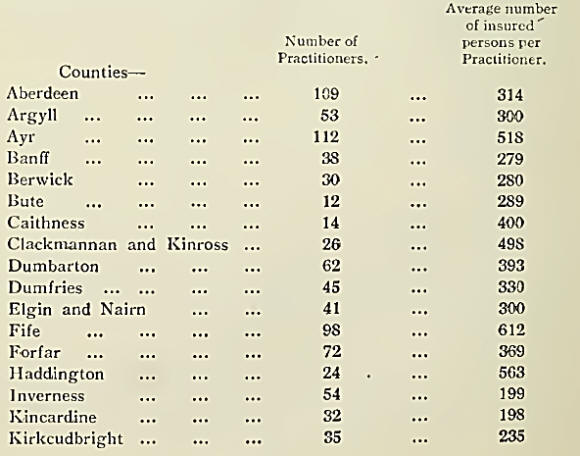
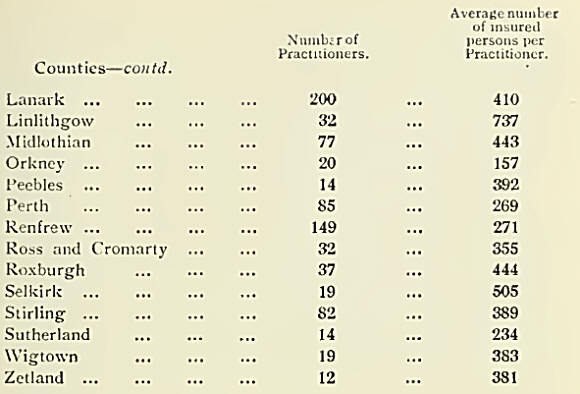

As regards the number of
persons receiving- attendance from each insurance service practitioner,
in five Counties there
are more than 500 insured
persons per practitioner, and in nine more than 100. Among- these, the
highest number is in Linlithgow, with an average of 737; the next in
order is Fife, with an average of 612. The remaining 22 county areas
have 400 insured persons or less per panel practitioner. Orkney,
Kincardine, and Inverness are all below 200.
In the burgh group the
majority of Burghs—21 in number —show between 400 and 1,100 insured
persons to each insurance service practitioner. Two burghs show less
than -100: Rutherglen with 255 on an average, and Wishaw with 274. Three
burghs show more than 1,000, namely Clydebank with 1,006, Paisley with
1,231, and Dundee with 1,638 insured persons, respectively, per
practitioner on the medical list.
Mileage.
Considerable discussion
has been aroused in Scotland among medical practitioners in country
districts as to their relative disabilities as compared with urban
practitioners, more especially the difficulty caused by sparseness of
population and deficiency of means of locomotion. It is now admitted
that the advent of the motor car has solved many of these difficulties,
although some expense is entailed by the upkeep of a car. The following
passage on mileage is taken from the Report of the Scottish Insurance
Commission :—
“Mileage is the distance
which has to be travelled by doctors in order to visit their patients.
It is that which has to be annihilated in order to place doctors who are
remote from insured persons on an equality with those who live closer by
them.”
The question of mileage
is not one of distance merely, though the distances travelled by doctors
in Scotland are often remarkable. It involves such further consideration
as deficiency or absence of roads, crossing of moors or mountains, and
frequently passage by water. It is closely related to economic
conditions, especially in the Highlands, of which it may be said that
wherever the doctor’s journeys are longest and most arduous, the means
to lighten the burdens of travel will be found to be least available.
At a Conference held on
25th and 26th November, 1912, between the Chancellor of the Exchequer
and a deputation from the British Medical Association, the subject of
financial provision for mileage, over and above the redistribution
permitted under the Medical Benefit Regulations, was put forward for
consideration. It was recognised by the Government that in some parts of
the country which are exceptionally sparsely populated, and in which
there are special difficulties of access (such as mountain, bog, and
moorland), practitioners would be placed at special disadvantage, and it
was decided to ask Parliament to provide a special fund to be applied by
the Insurance Commissioners in making increased provision for such
areas.
Thereafter, at a meeting
on 3rd January, 1913, which took place in London between the Chancellor
of the Exchequer, the Commission, and the Chairmen and Clerks of the
Scottish County Insurance Committees the subject was again under
discussion. A small Committee was formed consisting of the Chairman of
Renfrew County Insurance Committee, and the Vice Chairman and Clerk of
Lanark County Insurance Committee, to procure from the various Scottish
County Insurance Committees information which might be of value in
dealing with the question. Schedules of enquiry were drawn up and issued
by the small Committee through Clerks of County Insurance Committees to
doctors in County areas throughout Scotland. The doctors were asked to
furnish on these schedules an approximate statement of the miles which
would require to be travelled by them, the miles being measured from the
nearest available practitioner on the panel. Miles were to be regarded
as of two varieties, normal miles, that is to say miles beyond three
measured along a driving road ; and special miles, that is to say miles
beyond three of any of which a quarter or more could not be so
travelled, but only on foot, as on hill or moor, and exceptionally by
ferry. These returns were duly furnished, and, though somewhat
approximate and in a number of cases incomplete, they proved of
considerable service by indicating the numerical scope of the problem as
it presented itself in Scotland.
Lowlands.
Apart from the Highlands
and Islands, for the sparsely populated rural areas of Great Britain a
mileage fund of p£50,000 has been voted. The share of this fund which
will fall to Scotland, excluding the Highlands and Islands, is ^1G,000.
While the Highlands, for the purposes of the Medical Service Committee
were properly demarcated from the Lowlands on the ground of the
straitened circumstances of the people, it would nevertheless be
inaccurate to conclude that in sparseness of population, ruggedness of
contour, want of railway communication, difficulty of road transit, or
rigour of climate the Highlands cannot be matched by certain portions of
the area which, for convenience of reference, is here entitled the
Lowlands. The eastern extremity of the Grampian Range intrudes into
Banffshire and Aberdeen, and the highest summit but one in the British
Isles is situated in the latter county. The rigorous winters at
Tomintoul are well known. Strathdon, where the doctor has to travel by
sleigh for several months each year has already been referred to. The
conditions prevailing in Arran and in the Border and Southern Counties
have been under the notice of the Commission. The whole Lowland area
outside the towns is essentially sparsely peopled.
Precise details remain to
be ascertained. It is the purpose of the Commission to take immediate
steps to investigate Lowland mileage by an expeditious method. The
object of the enquiry will be to ascertain a basis for distribution of
the grant with a view to its apportionment among individual doctors as
speedily as possible.
By Regulation 50 of the
Medical Benefit Regulations, an Insurance Committee may, if they think
fit, make arrangements for a payment to practitioners on the panel in
respect of mileage, such payment, by Regulation *10 (3), being deducted
from the Panel Fund for disbursement among doctors who attend insured
persons resident at such distance as may be determined. The financial
procedure involved, though nominally a deduction, is in effect a
redistribution of a portion of the Fund for the benefit of medical men
who have distances to travel.
The provision referred
to, which is in addition to, and not in place of, the subsidy which will
be payable from the Treasury Grant for mileage, was adopted by agreement
between the Insurance Committees of Lanarkshire and Midlothian and the
medical practitioners of these Counties. It was decided that the sum of
2d. per insured person per annum should be reserved to form a County
Mileage Fund. It is intended that the rate of payment shall, as far as
practicable, be Is. Gd. per mile over three from the doctor’s residence,
measured along a driving road.
HIGHLANDS AND ISLANDS
MEDICAL SERVICE COMMITTEE.
In many respects
including National Insurance the Highlands and Islands of Scotland
constitute one of the most difficult administrative problems of the
whole of the United Kingdom. It should always be borne in mind that a
relatively small proportion of the Highland population is employed in
the sense of the Act and that a combination of difficulties exist which
is not to be found elsewhere in Great Britain. The following from the
Scottish Report presents a good idea of the problem :—
“On the 11th July last
the Highlands and Islands Medical Service Committee (of which the Deputy
Chairman of the Commission was a member and one of the Inspectors the
Secretary) was appointed to investigate conditions in the Highlands and
Islands. In the absence of a definite indication in the terms of
reference as to the exact area to which the enquiry was to be confined,
the Committee determined to take evidence from the counties of Argyll,
Caithness, Inverness, Ross and Cromarty, Sutherland, Orkney and
Shetland, and from the Highlands of Perthshire.
“In the Committee’s
Report, which was submitted on the 24th December last, the circumstances
which made medical provision in the Highlands and Islands a special
problem were stated to be as follows :—
(a) That on account of
the sparseness of the population in some districts, and its irregular
distribution in others, the configuration of the country, and the
climatic conditions, medical attendance is uncertain for the people,
exceptionally onerous or even hazardous for the doctor, and generally
inadequate.
(b) That the straitened
circumstances of the people preclude adequate remuneration of medical
attendance by fees alone.
(c) That the insanitary!
conditions of life prevailing in some parts render medical treatment
difficult and largely ineffective.
(d) That in default or
disregard of skilled medical advice and nursing, recourse is not
infrequently had to primitive and ignorant methods of treating illness
and disease. These methods are a source of danger, especially in
maternity.
(e) That there is danger
of physical deterioration from defective dieting, and more markedly in
the infant and juvenile population.
(f) That rural
depopulation is not a feature of the whole area of the remit, and thatl
even where notable, the necessity for medical provision is not
materially reduced.
(g) That the local rates,
from which the doctors’ income is mainly derived, are in many cases
overburdened.
(h) That owing to the
industrial conditions the Insurance Act is only very partially
operative.
(i) That, in short, the
combination of social, economic, and geographical difficulties in the
Highlands and Islands—not to be found elsewhere in Scotland—demand
exceptional treatment.
“The quality of the
country is specifically referred to as rugged, roadless and mountainous.
Where not composed of islands, it is described as very largely
peninsular on the seaboard, and broken up inland by lakes and rivers.
“Adverting to the
Insurance Medical Service, the Committee state that they are convinced
that the industrial conditions of the area are such as to make the
provisions of the Insurance Act less operative than in other parts of
Scotland, and they foresee considerable trouble in providing medical
benefit for fully-insured persons far removed from a medical centre.
They express the view that special subvention for the insured would
appear to be necessary, and that the provision of medical attendance for
their dependants is also a matter requiring urgent consideration. It was
clear to the Committee that, having regard to the economic conditions
prevailing in the Highlands and Islands, the extent to which medical
services are at present subsidised from Imperial funds is quite
inadequate, and that as local resources are in many parishes already
well nigh, if not wholly, exhausted, any general amelioration of the
existing medical service cannot be achieved without a further and a more
substantial subsidy.
“In subvention of the
Insurance Medical Service there was voted in the Special Grant-in-aid to
Scotland for 1912-13 the sum of ;£l0,000 for the Highlands and Islands
for mileage and other special charges. In order to make this money
available at the earliest possible moment to medical men in the
Highlands and Islands the Commission, through their Inspectors, are now
engaged in obtaining data to enable them to prepare a scheme for its
distribution on an equitable basis between the County Insurance
Committees concerned. For the purpose of enquiry, the provisional
standard is a three-mile limit from the residence of the nearest
available insurance service practitioner, but all sea journeys are being
noted, whether within or without three miles. The basis of distribution
to medical men within counties will be determined as soon as possible
after the enquiry is completed.
“It should be observed
that the ^10,000 is not for mileage only, but for special charges also.
These terms of the Grant, provided the fund suffices, will give an
opportunity to treat cases of exceptional hardship with the
consideration which they may be found to merit. Cases of difficulty and
danger in the medical service of the Highlands and Islands have come
under the observation of the Commission.”
It only remains to be
added in this connection that as a result of the National Insurance Act
and the investigations and recommendations of the Dewar Committee, an
Act has been passed to provide a special parliamentary grant of ^"42,000
a year to aid in improving the medical service in the Highlands and
Islands, and a special Board has been constituted to administer this
fund and to administer schemes for the improvement of the medical
service in the district concerned. Great hopes are entertained of a much
needed improvement in the medical service of the Highlands and Islands
of the North of Scotland.
CHEMISTS.
The provision and supply
of proper and sufficient drugs and medicines and prescribed appliances
to insured persons is one of the duties of every Insurance Committee.
No difficulty was
experienced in Scotland in arranging for this supply. Scotland has been
fortunate in having in the pharmacy profession an excellently trained
service who have deservedly won high reputation for skill and integrity.
Some attempts have been made in various quarters to suggest that some
Scottish chemists were supplying inferior drugs and medicines for the
use of insured persons. Not a shadow of proof was ever forthcoming for a
charge which is not now heard. On the contrary we have direct testimony
that Scottish chemists continue to dispense drugs and medicines of the
same high quality as they formerly supplied, and indeed as they were
bound to supply according to agreement and the law of the land. The
following- statement of the position of chemists is taken from the
Scottish Commission’s Report:—
“The position of chemists
in Scotland with respect to service under the Act is believed to differ
in some degree from that of their professional brethren in England. It
is understood that in the past throughout England generally the supply
of drugs to patients by medical men has been the prevailing custom, and
in certain districts the almost unbroken rule, not only in country
places where no pharmacist was established, but also in cities where the
services of chemists; could readily have been secured. In Scotland, on
the other hand, while doctors in remote and solitary places have
dispensed their own medicines, they have done so under the constraint of
circumstance, and the great majority of medical men in towns and other
populous areas have been content to leave the work to chemists.”
It is understood that in
England, as contrasted with Scotland, the amount of medicine consumed
per patient is higher; that the period for which mixtures are prescribed
to last is shorter, leading to more frequent repeats and consequent
dispensing fees; and that the proportion of mixtures, which are quickly
made up, to such preparations as pills and powders, which take some
time, is very considerably greater.
So it has come to pass
that the Act, by drawing a line of separation between medical treatment
and the provision of drugs, has directed into the hands of English
chemists an. increased volume of trade, without conferring upon Scottish
chemists an equal or corresponding advantage. It has been alleged by
pharmacists in Scotland generally that the Act cannot increase their
custom ; and on this ground, it is presumed, they have been disposed to
praise the tariff of charges somewhat faintly.
The Commission were
informed that investigations made by Pharmaceutical Committees and
others in important Scottish centres appeared to show that the tariff of
prices was likely to leave the Drug Fund of the areas concerned at the
close of the year with an appreciable balance to carry forward. A
supplement to the tariff was submitted by the Secretary of the
Pharmaceutical Standing'
Committee. The Commission let it be known that they were prepared to
approve the supplement, which rectifies certain inaccuracies. They also
said that, if at the end of twelve months it should be found that there
was an unexpended balance in the Drug Fund sufficient to justify an
additional proportionate retrospective payment not exceeding 10°/o on
the amount of the accounts of individual chemists, they would consent to
such additional payment being made as might be approved by themselves
and the Insurance Committee.
In reply to a request
that they would indicate their readiness to consider a stated case in
regard to an increase in dispensing fees, a general revision of tariff
prices, and payment for postage or carriage of medicines for insured
persons in rural areas, the Commission explained that while they would,
at any time, be glad to give careful consideration to such
representations, they would deprecate any amendments being made until a
year’s experience of the working of the tariff has been obtained. They
assumed that any proposals as regards revision of tariff prices had
reference only to an annual revision as at the date of the agreements,
and not to a scheme of adjustment of prices to follow market
fluctuations. Any suggestions on the last-mentioned lines they would
deem impracticable.
Representations were made
to the Commissioners by the Pharmaceutical Standing Committee (Scotland)
with respect to Regulation 30 (1) of the Medical Benefit Regulations, in
so far as it permits doctors to claim the right to supply medicines to
insured persons residing in a rural area more than a mile from the place
of business of a chemist who is on the list of an Insurance Committee.
The Standing Committee expressed the view that the Regulation, in so far
as it gives such permission, should be repealed. The Commission stated,
in reply, that they would afford every assistance to the Pharmaceutical
Standing Committee in submitting the special position in Scotland and in
explaining the difficulties which have been raised there by this
provision of the Regulation.
The procedure for dealing
with drugs, as opposed to appliances, in connection with pharmaceutical
service under the Act, was the occasion of frequent enquiries addressed
to the Commission.
By Regulation ‘28 of the
Medical Benefit Regulations, the Drug Tariff is the list of prices for
drugs ordinarily supplied and for prescribed appliances. There are other
drugs not on the Tariff, which may be ordered also, and the manner of
calculating payment for these is provided for in the Regulations ; but
there are no appliances permitted to be provided other than the
prescribed appliances, which by Regulation 27 are stated to be the
appliances mentioned in the Second Schedule.
The difficulties of
chemists in handling prescriptions ordered under this head were
appreciably increased by the circumstance that the tariff of prices of
appliances put forward by the Pharmaceutical Standing Committee was not
co-extensive with the Schedule. Splints, for example, are named in the
Schedule simpliciter; leg splints, therefore, may be ordered though arm
splints only are priced in the Tariff.
These considerations
ruled the decision as to the correct form to be used for ordering.
Prescriptions for drugs were to be entered on the green or pink form,
respectively, according as their component substances were or were not
all included among drugs priced in the Tariff; but all appliances
permitted to be ordered, whether priced in the Tariff or not, were to be
ordered on green forms. Appliances not included in the Second Schedule
to the Regulations were not to be ordered at all.
During the early days of
the operation of Medical Benefit, statements were circulated in certain
quarters to the effect that the pharmaceutical service of the Act was
such that insured persons must necessarily be supplied with drugs of an
inferior quality.
This statement is
incorrect. The conditions of the agreements entered into by chemists
with Insurance Committees expressly stipulate that all drugs shall be of
good quality, and any chemist failing to observe the terms of his
undertaking to the detriment of the service will be liable to have the
question of his continuance upon the list of chemists reported upon by
an Enquiry Committee appointed by the Commission.
Drugs duly ordered are to
be supplied to the insured persons by the chemist, the cost being
defrayed out of the Drug Fund at the prices set forth in the Tariff. It
is important to note that the Drug Tariff is not an exhaustive list of
the drugs which may be ordered for insured persons : it is a list,
prepared for the sake of convenience, showing the prices agreed to be
paid by an Insurance Committee for certain drugs if ordered. Drugs which
are not included in the Tariff, but which the doctor may consider
necessary for the proper treatment of the case are ordered in a special
manner, and their cost also forms a charge upon the Drug Fund :—
The number of chemists on
the lists of Insurance Committees in March, 1913, is shown in the
following table:—


|

